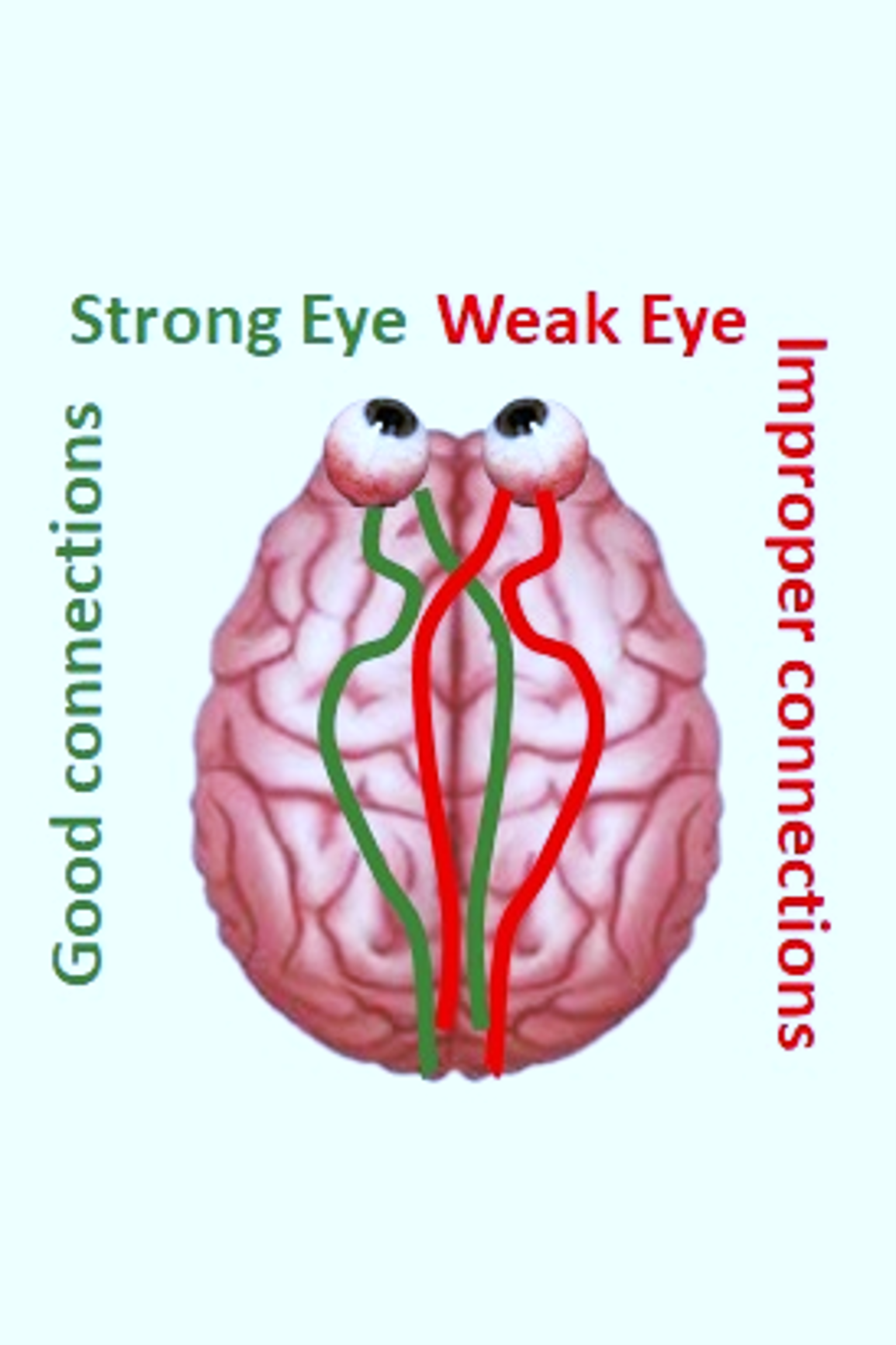
The term Amblyopia comes from Greek and it means “dullness of vision”. It is a visual disorder characterized by improper neural connections between one eye (the weak eye) and the brain, resulting in a heavy reliance on visual information from the other eye (the strong eye). “Levi et al. Vis. Res. 2015"
it is wide accepted a ocular suppression model of amblyopia. It considers binocular vision as a weighted sum of monocular inputs. In amblyopia the weight of the weak eye is decreased by the activity of the strong eye.
Amblyopia develops during early childhood (<7-8y), which is a crucial period for visual system development.
Risks Over time, the brain relies more and more on the strong eye while vision in the weaker eye gets worse Amblyopia can lead to lifelong impairment in the weak eye and lifelong impaired depth perception and associated fine motor skills. Amblyopia is associated to a risk of visual loss from 1.2% to 2.9%
Clinical assessment of amblyopia
Amblyopia impairs both monocular and binocular functions, and can be related to other anomalies like tropia and eccentric fixation
The most common clinical definition of amblyopia is based on the difference in visual acuity between the eyes, after best corrections for refractive errors, in absence of any physical impairment of the eyes.
A widely accepted difference is 2 or more Snellen or logMAR lines.
Other monocular visual functions are impaired in the amblyopic eye:
High frequencies spatial contrast (the narrowest black-and-white stripes that can be resolved);
vernier acuity (ability to detect small misalignments);
contrast sensitivity (ability to detect objects or patterns at different levels of contrast);
Amblyopia impairs the binocular functions with lack of stereopsis and poor stereocuity
Suppression tests assess whether the brain is suppressing visual input from one eye. Those include Worth 4-Dot test, Bangolini striated lens test (eventually including neutral filters), 4-diopter prism test, tests with polarized filters and binocular combination.
What causes amblyopia?
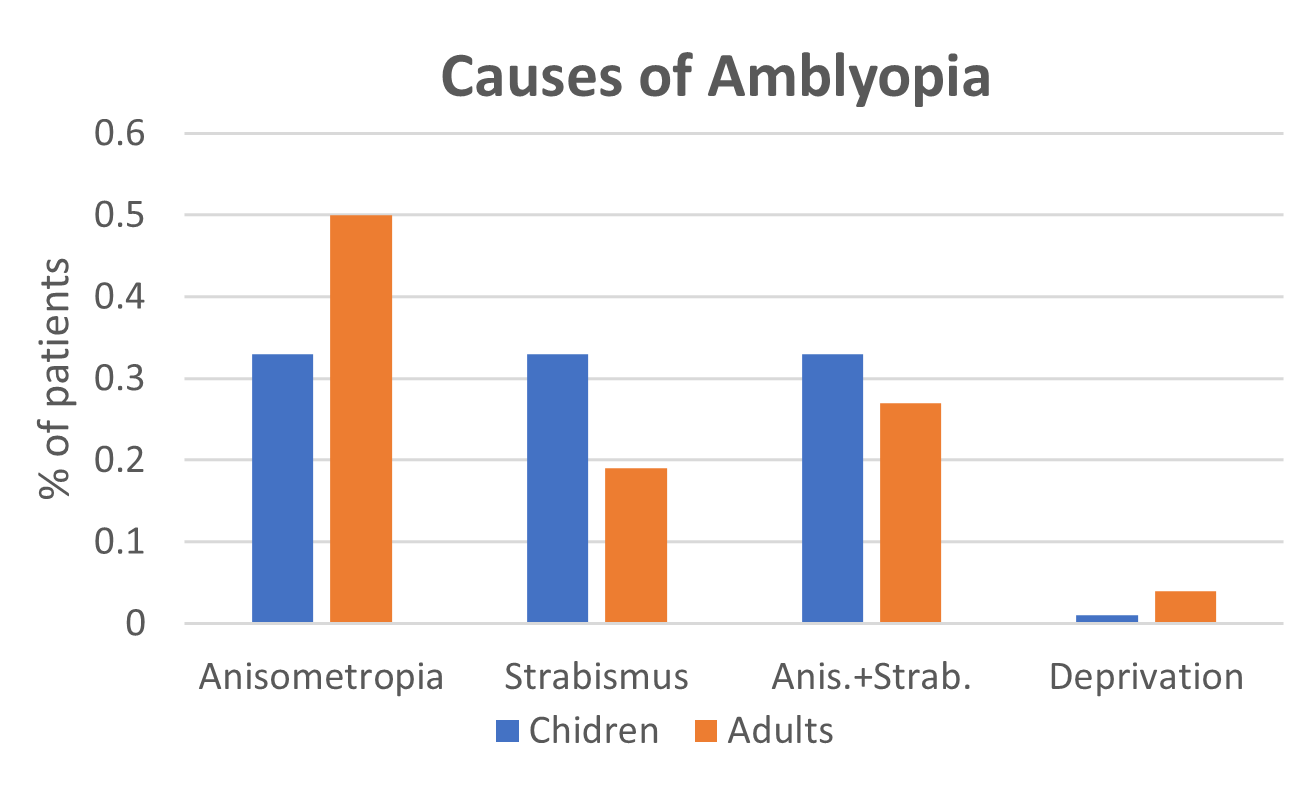
A complete clinical assessment of the oculomotor and visual system leads to diagnosis of one of three types of causes for amblyopia:
Animesotropia: the difference in visual acuity between the eyes
Strabismus: the eyes have an excess of misalignment.
Deprivation(rare):Cataracts (clouding of the lens of the eye) and Ptosi (partial palpebral lowering)
There are neural correlates of amblyopia?
Comparisons with non-amblyopic showed significant difference in the neural activities of retina , lateral geniculate bodies, visual and temporal cortex
What are amblyopia risk factors?
Were born early (premature)
Were smaller than average at birth
Have a family history of amblyopia
Have developmental disabilities
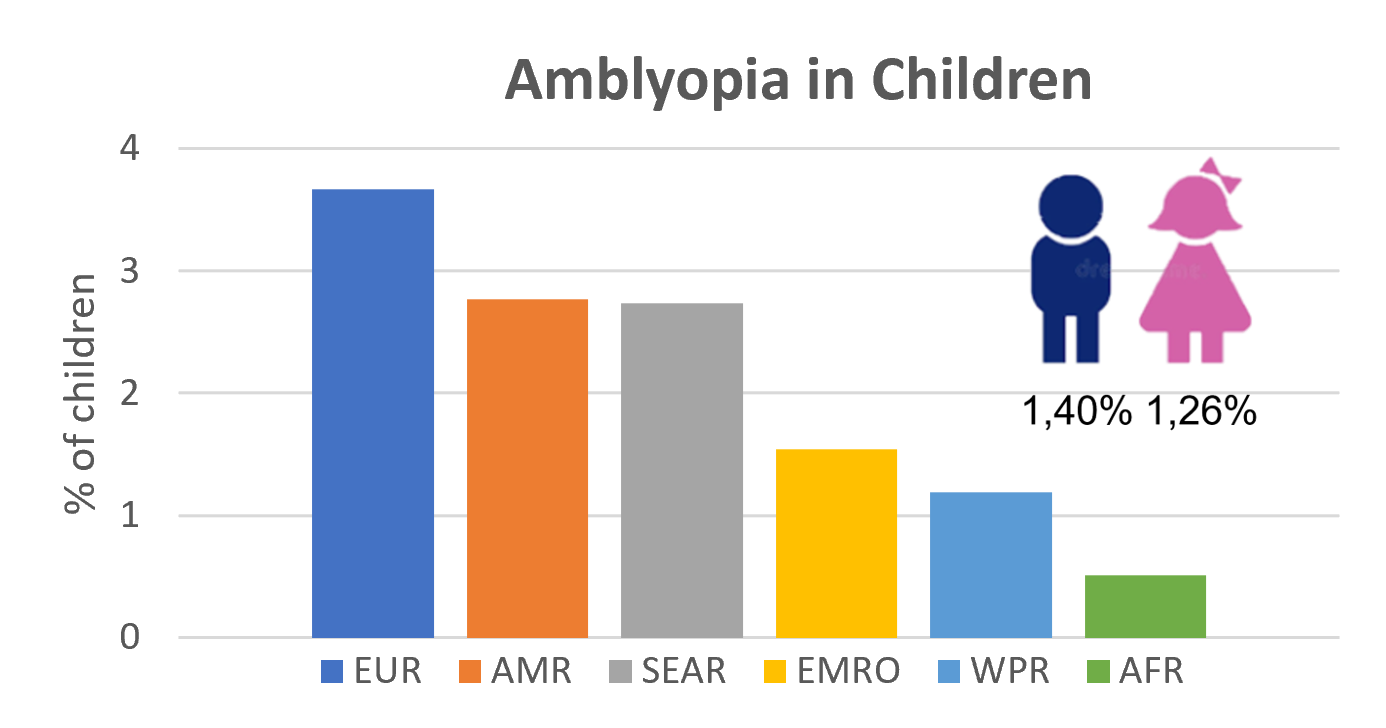
What is amblyopia prevalence in children?
The overall worldwide prevalence of amblyopia in children is about 1.36%, higher in in males (1.40%) than in females (1.24%).
The highest prevalence estimate is observed in Europe, the lowest in Africa (0.51%), but it is still unclear whether these differences are statistically significative.
In 2019 were estimated about 99 million people with amblyopia, estimate to encrease to 175 million by 2030 and 222 million by 2040.
How is treated amblyopia
Once recognized the type of Amblyopia, the first step is always to address the cause (e.g with refractive correction in animesotropia)
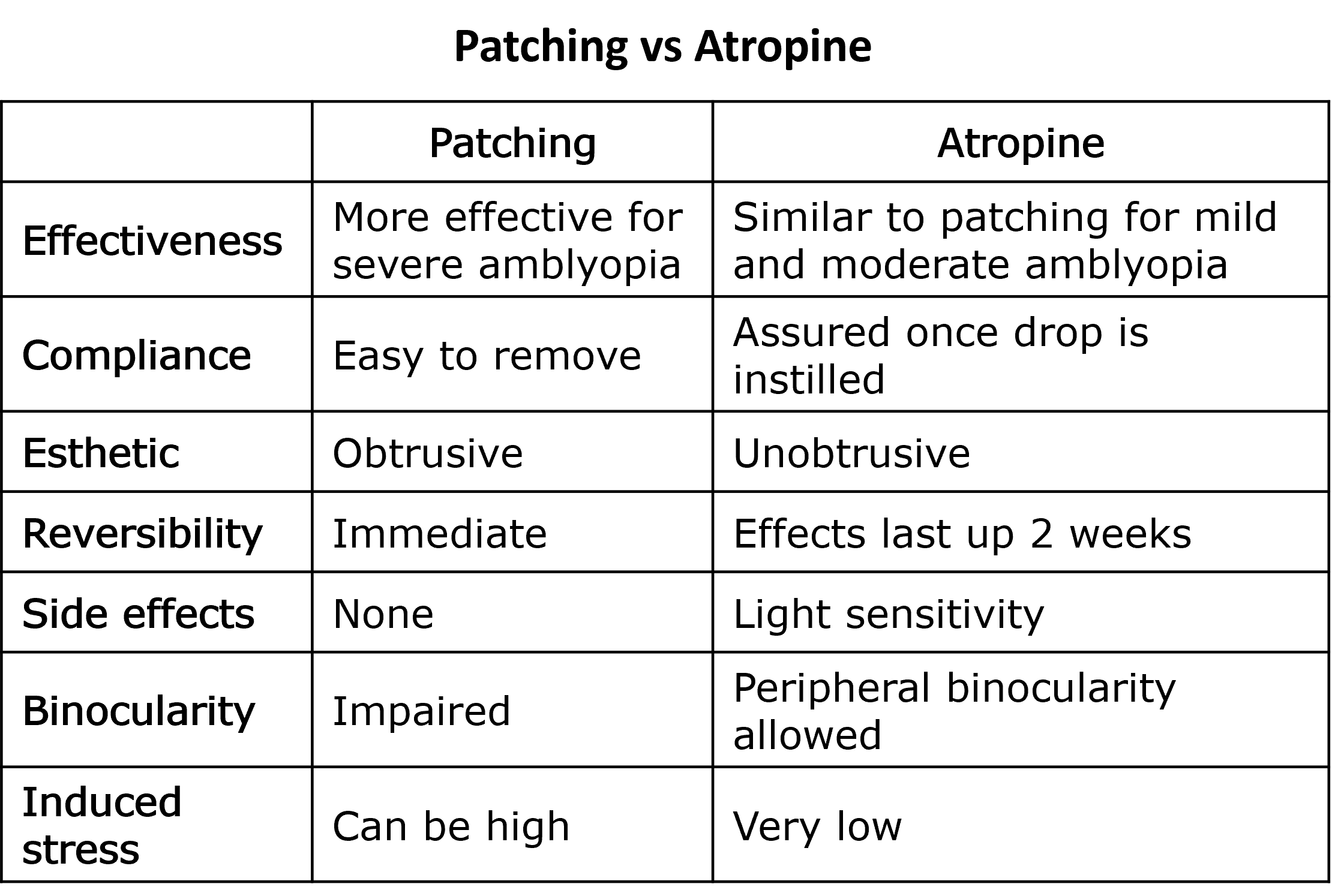
The best-established treatment for amblyopia is occlusion therapy, that consists in depriving the healthy eye of visual input by patching or by optical or pharmaceutical penalization(atropine).
Recently also amblyopia digital treatments become popular.
Patching
According to the severity of amblyopia the strong eye is patched for a variable amount of time: